
What is the Importance of Folic Acid during Pregnancy?
Folic acid, or folate (vitamin B9), is an essential nutrient for our health. It is necessary for DNA formation and a series of enzymatic reactions involved in amino acid production and vitamin metabolism.
During pregnancy, the body’s demand for folate increases considerably, since this vitamin is also necessary for the fetus’s growth and development. Folic acid deficiency during pregnancy is associated with severe fetal abnormalities, particularly those referred to as neural tube defects (NTD).
Abnormalities in neural tube formation are the second most common cause of fetal malformation, surpassed only by congenital heart diseases.
The neural tube is an embryonic structure that gives rise to the spinal cord, vertebrae, meninges, brain, and skull. Defects in the fetal nervous system’s formation typically occur in pregnant women with unsatisfactory folic acid levels in their bodies during pregnancy.
This article will explain why folic acid supplementation is an essential preventive measure during pregnancy.
Note: The terms “folic acid” and “folate” are often used synonymously, but they are not exactly the same thing. Folic acid is the synthetic form of folate, also known as vitamin B9.
What are Neural Tube Defects?
Defects in neural tube formation can lead to various fetal malformations, such as:
Anencephaly: partial absence of the brain and skull cap.
Spina bifida: malformation of the spinal cord, in which some vertebrae do not form completely, allowing part of the spinal cord to project through the opening in the bones.
Encephalocele: a defect in which the brain and meninges herniate through openings in the skull.
Structural problems resulting from neural tube defects are often severe and without definitive treatment. When they do not result in the baby’s death, they usually cause significant disability.
One of the leading causes of neural tube malformations is folate deficiency during pregnancy. Therefore, it is unsurprising that this malformation can be prevented with folic acid supplementation.
However, a significant problem makes the solution more complex than it seems: the neural tube forms in the first four weeks of embryonic life. Since most women only discover they are pregnant after at least five or six weeks of gestation, the neural tube formation process is usually completed by the time the pregnancy is diagnosed. After the 6th week of gestation, the preventive action of folic acid is much less effective.
Therefore, every woman planning to become pregnant should start taking folic acid at least one month before getting pregnant to ensure satisfactory blood levels during the formation of the fetal nervous system.
What is Folic Acid?
Folic acid is a vitamin from the vitamin B family, necessary for DNA synthesis and new cell production. During pregnancy, a woman needs sufficient amounts of folic acid for herself and the developing fetus.
Folate is found naturally in foods such as spinach (60 mcg/100 g), lettuce (40 mcg/100 g), broccoli (100 mcg/100 g), beans (100-300 mcg/100 g), cereals (varies depending on the product), Brussels sprouts (60 mcg/100 g), potatoes (20 mcg/100 g), brown rice (49 mcg/100 g), fruits like oranges (30 mcg/100 g) and bananas (20 mcg/100 g), and liver meat (300 mcg/100 g).
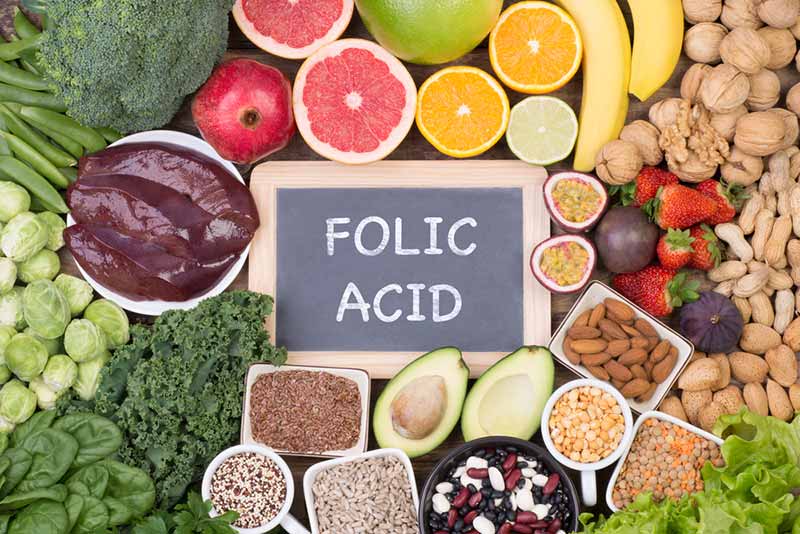
In many countries worldwide, various foods receive folic acid supplementation, including cereals like rice, wheat, and corn. The folic acid values mentioned above may be even higher in artificially enriched foods.
In the United States, the FDA (Food and Drug Administration) has recommended folic acid supplementation for all cereals since 1998. This simple measure has reduced the incidence of neural tube defects in the country by 50%.
Folic acid is essential in preventing neural tube defects and promoting fetal growth, so it should be consumed before and throughout pregnancy.
Deficiency
Although folic acid is a vitamin naturally found in various foods, utilizing artificial supplementation is a more effective strategy for preventing neural tube defects. The reason for this lies in the significantly enhanced bioavailability of folic acid derived from supplements or artificially fortified foods compared to the bioavailability of folate obtained through natural food sources.
A study conducted in the United States between 2007 and 2012 (National Health and Nutrition Examination Survey) showed that up to 1 in every 4 American women had folic acid levels below the recommended amount. Several factors can explain this high number, including:
- Low-carbohydrate diets can lead to folate deficiency since bread and pasta are made with fortified grains.
- Increased consumption of foods designated as “organic,” which do not receive artificial folic acid supplementation.
- Malnutrition.
- Diseases and medications that reduce folate levels (explained in the next section).
Folic acid supplementation before and during pregnancy significantly helps reduce the risk of neural tube defects; however, it does not eliminate the risk entirely. Situations such as poorly controlled diabetes, chromosomal defects, and obesity are also associated with a higher risk of neural tube problems.
Folic acid supplementation is estimated to prevent approximately 50 to 70% of neural tube defect cases.
Which women are at higher risk of having a baby with neural tube defects?
Pregnant women with the following conditions or characteristics are at higher risk:
- Women who have already had a child with a neural tube defect.
- Family history of neural tube defects.
- Women taking anticonvulsant medications (examples: valproic acid, carbamazepine, phenytoin, or phenobarbital).
- Women taking medications that reduce the availability or activity of folic acid (examples: triamterene, sulfamethoxazole-trimethoprim, metformin, or sulfasalazine).
- Diabetes mellitus.
- Sickle cell anemia.
- Celiac disease.
- Crohn’s disease.
- Other medical or surgical conditions that cause gastrointestinal malabsorption.
- Smokers.
- Women with a history of alcoholism.
What is the appropriate daily dose of folic acid?
For many women, dietary intake alone may not suffice in maintaining optimal levels of folic acid during pregnancy. As a safety measure, supplementation is advised for all pregnant women and those intending to conceive.
In fact, considering that up to half of all pregnancies are unplanned, it is prudent for women of childbearing age to pay attention to their folic acid consumption.
The recommended minimum daily folic acid dose for expectant mothers ranges from 0.4 to 0.6 mg. Tablets on the market vary from 0.2 mg to 15 mg. The 5 mg folic acid tablet is the most common and more than adequate for replenishing a mother’s reserves.
Women with a higher risk of having a child with neural tube defects may require higher doses of folic acid supplementation. The highest dose (1 to 4 mg daily) should be initiated one to three months prior to conception and maintained at least throughout the first 12 weeks of pregnancy. Subsequently, the dose should be reduced to 0.4 mg and continued until four to six weeks postpartum or until breastfeeding is completed.
Consistent and daily supplementation is crucial in ensuring sufficient folic acid intake.
Drug interactions
Folic acid may interact with certain medications or substances. Common interactions include:
- Fluorouracil products: Folic Acid may enhance the adverse/toxic effect of fluorouracil products.
- Phenytoin: Folic acid may lower the blood concentration of phenytoin.
- Green tea: The blood concentration of folic acid may be decreased by green tea consumption.
- Phenobarbital: Folic acid may reduce the blood concentration of phenobarbital.
- Primidone: Folic acid may decrease the blood concentration of primidone, as well as the concentrations of primidone’s active metabolites (e.g., phenobarbital).
- Pyrimethamine: The therapeutic effect of pyrimethamine may be diminished by folic acid.
- Sulfadoxine: Folic acid may impair the therapeutic effect of sulfadoxine.
- Sulfasalazine: The blood concentration of folic acid may be reduced by sulfasalazine.
Frequently Asked Questions
How long should I take folic acid during pregnancy?
Ideally, folic acid should be taken at least 30 days before conception and continued until the end of the first trimester (12 weeks of pregnancy). If you have previously had a child with a neural tube defect, supplementation should begin at least 3 months before attempting another pregnancy.
When is the best time to take folic acid?
There is no specific time for taking folic acid. If you are taking a folic acid supplement with iron, it is recommended to take it 30-60 minutes before a meal to increase absorption and reduce adverse effects. However, if you forget to take it before a meal, it is fine to take it at another time.
What are the consequences of not taking folic acid during pregnancy?
If you have a folate deficiency, which occurs in 20-25% of women, the fetus may develop neural tube defects such as anencephaly, spina bifida, or encephalocele.
Is it safe to take folic acid until the end of pregnancy?
Yes, there is no problem with continuing folic acid supplementation throughout pregnancy. However, the first trimester is the most crucial period for preventing neural tube defects.
Do folic acid and ferrous sulfate serve the same purpose?
No, they are different elements. Folic acid replenishes folate, and ferrous sulfate replenishes iron.
Can folic acid help prevent other complications during pregnancy besides neural tube defects?
Folic acid supplementation may offer additional benefits during pregnancy unrelated to preventing neural tube defects or anemia. However, the available data do not support a clear benefit for most other obstetric complications.
Can folic acid supplementation during pregnancy prevent autism in children?
Four of five recent meta-analyses of observational studies have linked folic acid supplementation to a lower risk of autism spectrum disorder. However, the included studies were of low quality, and the data are insufficient to justify changing recommendations for folic acid supplementation. Currently, no randomized studies are available on this subject.
I discovered I am pregnant but haven’t been taking folic acid; is there a risk?
There is always a risk, but starting supplementation within the first few weeks of pregnancy significantly reduces this risk.
Are there any contraindications for using folic acid during pregnancy?
No, there are no general contraindications. However, for those with epilepsy, folic acid may interfere with the efficacy of some anticonvulsant medications. In such cases, adjustments in doses and medications may be necessary.
Is it necessary to monitor folic acid levels during pregnancy?
In most cases, monitoring folic acid supplementation with blood tests is unnecessary, as studies have shown that simple daily supplementation is sufficient for 99% of pregnant women to achieve adequate blood folic acid levels.
Some specialists recommend that women with folate deficiency due to a known comorbidity (such as inflammatory bowel disease or bariatric surgery) should be monitored with monthly evaluations to ensure proper supplementation (blood folate level of 28-30 nmol/L). However, there is not enough evidence to support or refute this practice.
Is it possible for my baby to have a neural tube defect despite correct folic acid supplementation?
Yes, although uncommon, it can happen. The incidence of neural tube abnormalities, despite high-dose folic acid supplementation (4 mg), is 1%. These cases likely occur due to factors such as autoantibodies to folate receptors, malformations arising independently of folate levels, such as aneuploidy, poor glucose control in diabetic pregnant women, first-trimester hyperthermia, and specific genetic syndromes.
References
- Folic Acid Supplementation and Pregnancy: More Than Just Neural Tube Defect Prevention – Reviews in obstetrics and gynecology.
- Daily iron and folic acid supplementation during pregnancy – World Health Organization (WHO).
- Folic Acid – Centers for Disease Control and Prevention (CDC).
- Effectiveness of folic acid supplementation in pregnancy on reducing the risk of small-for-gestational age neonates: a population study, systematic review and meta-analysis – Royal College of Obstetricians and Gynaecologists
- Strategies for Preventing Folate-Related Neural Tube Defects: Supplements, Fortified Foods, or Both? – JAMA
- Folic acid supplementation in pregnancy – UpToDate.
Author(s)
Médico graduado pela Universidade Federal do Rio de Janeiro (UFRJ), com títulos de especialista em Medicina Interna e Nefrologia pela Universidade Estadual do Rio de Janeiro (UERJ), Sociedade Brasileira de Nefrologia (SBN), Universidade do Porto e pelo Colégio de Especialidade de Nefrologia de Portugal.





